
Facial masking: how much do we know about it in Parkinson’s disease?
9/20/24, 10 mins reading

Facial masking is used in Parkinson’s disease (PD) to describe the reduction or lack of facial expression (blank expression).
The facial expression includes spontaneous facial movements and emotional facial movements. it can occur as early as stage 1. The symptoms are pretty common and can vary from a decrease in blinking rate, diminished lower face, and perioral movement to the parting of lips all the time, which presents a masked face. On the one hand, facial masking can be treated as motor symptoms, on the other hand, facial masking is also implicated in non-motor symptoms such as cognitive impairment, mood disorders, and pathological social behaviors. Unlike motor symptoms on the limbs in PD, the symptoms of facial masking are usually symmetrical.
Diagnosis
Unified Parkinson’s Disease Rating Scale
Many methods have been developed to assess the presence and severity of facial masking. The most used one was the Unified Parkinson’s Disease Rating Scale (UPDRS) created in 1987, in which facial expression was graded with 5 levels based on the overall expression of the face and parting of lips. In 2008, the eye-blink frequency was adopted and added to this assessment system by the International Movement Disorder Society-Unified Parkinson’s Disease Rating Scale (MDS-UPDRS)
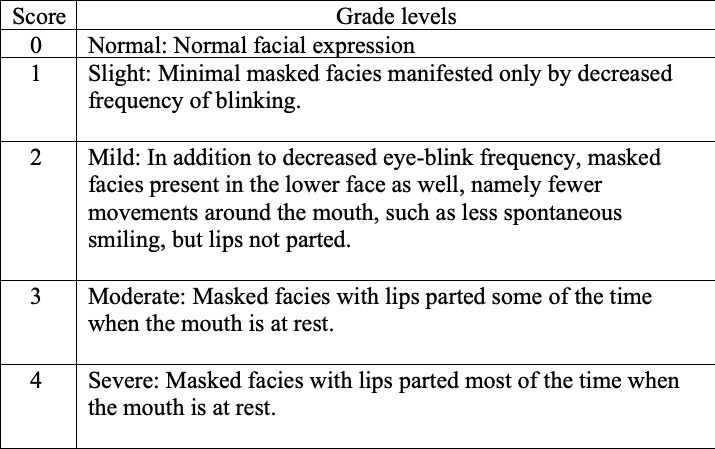
Table: A scoring system updated by MDS-UPDRS in 2008
Other methods
The MDS-UPDRS scoring system has been used for most clinical assessments of facial masking in PD. However, due to the shortcomings of this system such as the subjectivity of assessors and the lack of sensitivity, Clinicians have been exploring alternative methods to quantify facial masking.
One of these is electromyography(EMG), which measures and analyzes muscle activity after nerve stimulation. Besides, facial video and image with the help of artificial intelligence are also being assessed to diagnose and quantify facial masking in PD patients. With the advent of big databases and applications of artificial intelligence, it is believed that the diagnosis and grading of facial masking in Parkinson’s disease will make great progress very soon.
Mechanism
The specific pathophysiological mechanism of facial masking remains unknown and the consensus in the research community is that there are multiple brain regions, pathways, and networks involved. Here are some key notes regarding the mechanism of facial masking:
A variety of cortical areas of the human brain including motor, premotor cortices, supplementary motor area, and a mesial are involved with facial motor control.
The upper and lower parts of the facial movements are controlled by different motor systems.
Voluntary and involuntary facial movements are controlled by different neural pathways with an extent of overlapping.
Spontaneous movement such as eye blinking is associated with the dopaminergic system. One of the indicators is that the reduction of eye blinking rate is associated with the severity of bradykinesia and rigidity. Besides, the symptom of low eye blinking rate is improved after L-DOPA treatment.
There are also overlapping regions in the brain between the emotional movement-controlling area and the facial movement-controlling area, which allows the transition of motor activation to emotional movement.
Treatments
Dopamine.
The mechanisms underlying facial masking are extremely complex and are involved in multiple brain regions and networks. Nonetheless, dopamine treatment is showing a great amount of promise for facial masking in PD. One study has revealed that there is an association between facial masking and other motor symptoms such as rigidity and bradykinesia in terms of severity. Secondly, a study has also demonstrated that the severity of facial masking is correlated with that of nigrostriatal dopaminergic degeneration. More recently, a treatment experiment illustrated that PD patients treated with dopamine presented significant facial expression improvement than those without dopamine treatment. All these data showed that dopamine treatment has held the key to the management of facial masking in PD.
Physiotherapy, speech therapy, brain stimulations.
Besides dopamine, non-pharmacological treatments such as speech therapy, physiotherapy, or brain stimulations also present the potential effect and efficacy as complementary treatments.
Summary
The mechanism underlying facial masking in PD is rather complex and remains to be dissected fully. However, the diagnosis and grading of facial masking is expected to make a big progression, especially with the increasing capabilities of video and image technology from artificial intelligence development. With regard to treatments, dopamine undoubtedly remains the major medication while other treatments such as speech therapy, and brain stimulations are still in the process of developing as complementary ones.
More reading:
Masked Faces in Parkinson's Disease: Mechanism and Treatment
The Story Behind the Mask: A Narrative Review on Hypomimia in Parkinson’s Disease
LSVT LOUD: Speech Therapy for Parkinson’s Disease